
Page 15 - Roche Hemlibra Non-inhibitors - Product Monograph
P. 15
Severe Moderate
100
90
80 22 31
3
5
70 9 5 2
Median HJHS 50 15 50 7
60
40
30 58 n=0 moderates on prophhylaxis
18
20
10 10
40 51
0
od p od p od p od p
0-18 19-39 40-59 60 and above
Age (y)
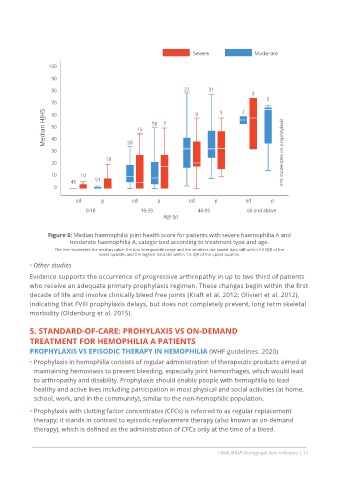
Figure 6: Median haemophilia joint health score for patients with severe haemophilia A and
moderate haemophilia A, categorized according to treatment type and age.
The line represents the median value; the box interquartile range and the whiskers the lowest data still within 1.5 IQR of the
lower quartile, and the highest data still within 1.5 IQR of the upper quartile.
• Other studies
Evidence supports the occurrence of progressive arthropathy in up to two third of patients
who receive an adequate primary prophylaxis regimen. These changes begin within the first
decade of life and involve clinically bleed free joints (Kraft et al. 2012; Olivieri et al. 2012),
indicating that FVIII prophylaxis delays, but does not completely prevent, long term skeletal
morbidity (Oldenburg et al. 2015).
5. STANDARD-OF-CARE: PROHYLAXIS VS ON-DEMAND
TREATMENT FOR HEMOPHILIA A PATIENTS
PROPHYLAXIS VS EPISODIC THERAPY IN HEMOPHILIA (WHF guidelines. 2020)
• Prophylaxis in hemophilia consists of regular administration of therapeutic products aimed at
maintaining hemostasis to prevent bleeding, especially joint hemorrhages, which would lead
to arthropathy and disability. Prophylaxis should enable people with hemophilia to lead
healthy and active lives including participation in most physical and social activities (at home,
school, work, and in the community), similar to the non hemophilic population.
• Prophylaxis with clotting factor concentrates (CFCs) is referred to as regular replacement
therapy; it stands in contrast to episodic replacement therapy (also known as on demand
therapy), which is defined as the administration of CFCs only at the time of a bleed.
HEMLIBRA Monograph-Non-inhibitors | 13
®